World
There’s a dilemma at the heart of the NHS – but politicians don’t want to talk about it | Adam Boulton



Margaret Thatcher’s sometime chancellor Nigel Lawson famously remarked that the NHS is “the closest thing the English people have to a religion”.
Certainly, as the UK census records a decline in adherence to Christianity, celebrating and bemoaning the state of “our NHS” brings together citizens of all creeds and political persuasions.
Everyone fears pain and sickness. The aspiration of those who set up the NHS was to divorce those real concerns from worries about money and being able to pay for care.
The NHS was to be paid for through taxation, making all treatment “free at the point of delivery”.
For many people, the idea that health care should not be paid for by the individual has become an article of faith.
This week, the inference that he’d gone against this rule provided an effective line of attack against the prime minister, who also happens to be a multimillionaire.
After days of challenge from the media and political opponents, Rishi Sunak finally confessed at PMQs that he had “used independent health care in the past”, while protesting “I am registered with a NHS GP”.
If you are an NHS worker and would like to share your experiences with us anonymously, please email NHSstories@sky.uk
‘I have used independent health care in past’
What does ‘free’ really mean?
In reality, the divide between “free”, taxpayer-funded health care, and good, private medicine is nowhere near as clear-cut as Mr Sunak‘s awkward moments would suggest.
The majority of NHS users actually make some sort of personal “co-payment” for services, every time they pick up a prescription.
According to the Office of National Statistics, at least 13% of adults paid for private medical care in the last year.
And just to keep up with present inadequate levels of treatment, the NHS itself is heavily reliant on contracting workers and services from the private sector.
Read more:
‘Climbing over people… blood in the floor’
Nurse suffers miscarriage after five-hour A&E wait

‘I couldn’t believe what I was seeing’
When the NHS was established in 1948, the official leaflet sent out to all households spelt out its core principles.
“Everyone – rich or poor, man, woman or child – can use it or any part of it,” it said.
“There are no charges, except for a few items. There are no insurance qualifications. But it is not a ‘charity’. You are all paying for it, mainly as taxpayers, and it will relieve your money worries in time of illness.”
From the start, that sidebar phrase “except for a few items” gave away that not everything would be absolutely free.
Some services would require some payments by some patients.
Nye Bevan, the minister who launched the NHS, resigned from the Labour government when charges were introduced for “teeth and specs” – dental treatment, dentures, glasses and surgical appliances.
A few years later, a Conservative government introduced prescription charges. All these still apply today, even as the cost of health care for the nation has multiplied 10 times over.
The NHS budget in 1948 was £437m – the equivalent of some £16bn in today’s money.
The NHS budget for 2023-24 has been set at £160.4bn, subject to any subsequent emergency funding to deal with strikes and the “health care crisis”.
Read more:
A&E waits hit new high
Worst region in England for handover times

Health Secretary Aneurin Bevan launched the NHS in 1948
From GPs to social care, NHS setup is full of anomalies
There are further anomalies in the way the NHS is set up: family doctors are supposed to be the gateway to treatment in the NHS – but GPs stayed out of the system. Their practices are self-employed small businesses, while in hospitals; doctors, nurses, and technicians are employed by the NHS.
Technically, taxpayers don’t pay directly to the NHS, but contribute to the budget for “health and social care services”.
But social care – looking after people who need it at home or in care homes – was excluded from the “free” principle and consequently underfunded.
With a growing proportion of elderly people in the population, the absence of properly funded care has resulted in alleged “bed blocking” at hospitals and inadequate pay for care workers compared to those doing a similar job in the health service.
Attempts by various governments to find ways for families to contribute more to the cost of care backfired. In 2017, Theresa May’s care proposals were quickly dubbed the “dementia tax”. An earlier plan from Labour was branded the “death tax” by Tory finance spokesman George Osborne.
Read more:
Are NHS failings to blame for extra deaths?
What happens to the body while waiting for an ambulance?

‘Nothing has changed!’
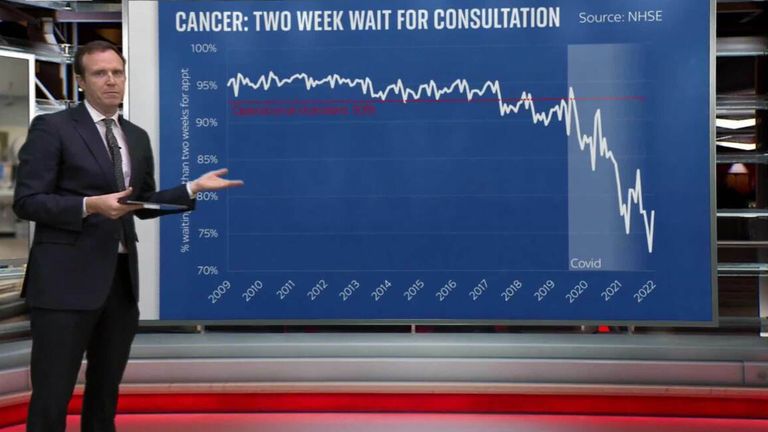
In the meantime, more than seven million people are on waiting lists for NHS treatment.
Waiting times are mounting in A&E departments and for ambulances delivering patients to hospitals. Britain’s “excess deaths” are running significantly above the average.
Once again, the relationship between the NHS and private health care is being seen as a solution by some and a problem by others.
Some NHS hospital trusts are buying operations for their patients in private hospitals – or even in French hospitals.
The government is planning to “buy” beds in care homes to get people out of hospitals.
On the other hand, some trusts are telling those on waiting lists that they can get their operations quickly if they go private – often using facilities in the same hospital, with the same NHS staff moonlighting.
Statistics suggest that overall delivery by NHS services was best during the early years of this century, after Tony Blair and Gordon Brown raised funding for the NHS to the European average for health care spending per capita.
Since then, the UK has dropped behind again.
Using OECD data, the King’s Fund reported that compared to most of the rest of the Western world, the UK has one of the lowest numbers of doctors, nurses, and hospital beds for the size of its population.
Read more:
NHS ‘clearly not working’
Pharmacy boss warns of shortages
Will the public pay more?
Argument continues over whether it is lack of funding or inefficient bureaucratic organisation which is responsible for the NHS crisis.
The public’s belief that health care should be “free” is not making a solution any easier. Opinion polls show public sympathy for the pay claims of nurses, doctors, and paramedics and for paying more for the NHS.
But this generous spirit does not extend very far in practice.
In a detailed survey by Redford and Wilton Strategies, asking “how much more in tax would the British public be prepared to pay to provide more funding to the NHS”, 43% said they would pay nothing more, and 24% set the maximum extra at £100. Only 11% said they would pay upwards of £500.
Read more:
‘I’ve never seen anything like this’
NHS workers describe daily ‘firefight’
Does Labour have a serious solution?
Labour says the extensive “NHS Plan” outlined by Sir Keir Starmer and Wes Streeting would be paid by ending non-dom status and without troubling most UK taxpayers.
This is highly ambitious since Labour proposes ending staff shortages by doubling the number of medical school places and of district nurses; 10,000 extra nurses and midwives each year and 5,000 more health visitors.
Nor is it clear how these long-term supply side measures would “end the Tory crisis”, as Sir Keir claims.
In its 75-year history, the NHS has been managed by both Labour and Conservative governments, and they have confronted the same challenges.
True, in most years since the 2008 banking crisis the NHS has been funded at below the average 4% annual increase it had come to expect since the 1950s.
But in that time, funding levels were never a major point of difference between the parties.
Read more:
How many spare beds does your local hospital have?
New COVID variant is fastest-growing strain in the UK
Health check for the NHS
Behind the rhetoric, the latest attempts to sort out the NHS are cross-party.
The government has appointed Patricia Hewitt, a former Labour health secretary, to conduct a review of the new integrated care boards. Both parties are developing long-term training programmes to end staffing shortages.
But the “free” NHS is so popular that politicians shy away from questioning its core principles and organisation, even though health care needs and available treatments are vastly different from those in 1948.
Voters want more and more without having to pay more for it. Rather than confront patients or health professionals with this dilemma, it’s easier to polish old grievances and indulge in a shouting match about those, including Mr Sunak, who can pay for health care bypassing the NHS which others cannot afford.