UK
90-second treatment for heavy periods leaves some women in agony – and needing a hysterectomy



Thousands of women every year have an endometrial ablation on the NHS.
It’s a treatment for heavy periods – and for a lot of women, the 90-second procedure brings relief from the sapping cycle of heavy bleeding.
But the procedure to destroy the womb lining fails in up to a fifth of cases, often leaving women with no treatment options left but a hysterectomy.
People whose ablations have failed describe debilitating, long-lasting pain that fractures mental health, relationships and careers – and doctors who seem to have little idea what’s wrong with them.
Karen Ramage knew immediately after her endometrial ablation in 2021 that something wasn’t right.
The pain only got worse. The month prior, she had run 100 miles. By two weeks after the procedure, she couldn’t walk properly. She couldn’t drive, she couldn’t work, she could barely eat. And she couldn’t find a doctor who would agree the endometrial ablation might be to blame.
“My personal belief is that they just don’t expect anything to go wrong,” she told Sky News.
The discussion of risks beforehand was limited to being warned of adhesions between the womb and bladder or bowel, she says. She was told the worst outcome would be no improvement in her bleeding.
But constant pain set in down her right side, intensifying to “labour-like contraction pains” around the time of her period.
As months passed, she relied on daily doses of Tramadol. Talking to a counsellor, she tried to reckon with how she could live like this: “I felt that everything had been taken away from me.”
Karen Ramage had to pay for a hysterectomy privately after her ablation failed
It took going private for a doctor to tell her definitively her ablation had failed.
“I was probably more relieved that actually somebody would believe in me, because it was this whole thing that nobody would believe that this procedure had caused all of this.”
Facing up to a two-year wait on the NHS for a hysterectomy, she took out a loan to cover the £7,500 cost of having it privately. After months not working, it was a tough financial call – one that meant relying on food banks.
How ablations work – and fail
About one in four women suffer from heavy periods and more than 30,000 women in England had an endometrial ablation on the NHS between 2017 and 2022.
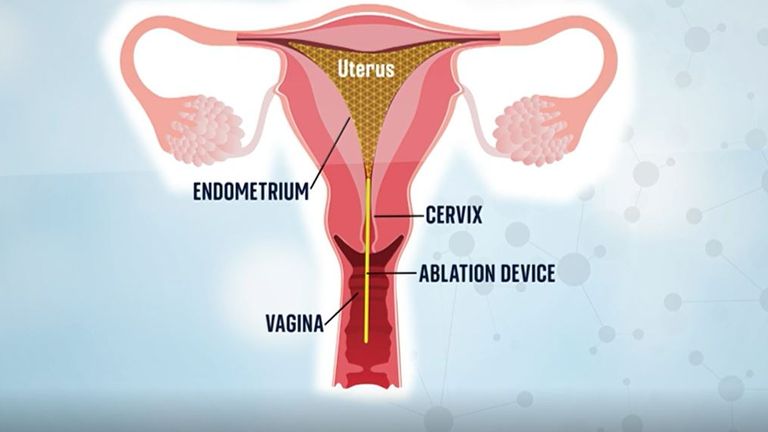
Most were radiofrequency ablations, where electromagnetic energy is used to burn away the lining of the womb.
The womb lining is what grows and sheds each month so the idea is that no lining means no – or lighter – periods.
But if not all the lining is destroyed, it still grows and sheds – but scar tissue can mean the blood gets trapped. It builds up in pockets behind the tissue, sometimes behind a scarred-shut cervix, causing intense pain until it disperses back into the body.
In women who have been sterilised the blood can back up into the fallopian tubes – this is known as PATSS (post-ablation tubal sterilisation syndrome).
In cases of late-onset failure, the lining regrows in the months and years after an ablation.
Some women experience pain cyclically each month, while for others post-ablation pain is constant or just during sex.
Women who spoke to Sky News describe agony worse than labour. One woman would put herself in the recovery position when the pain started because she knew she would blackout. Another came close to losing her job because she needed drugs so strong they made her a “zombie”.
‘Ablation ruined 10 years of my life’
Amanda Connor was told an ablation would “solve all my problems”, but three years later her womb had “completely grown back”. She decided to try the procedure a second time in 2010.
The pattern of monthly pain only intensified over time. It would start in her feet, a tingling fiery burn. By the time it reached her legs, she would be doubled over. Then it raged through her abdomen.
“I couldn’t stand up, I was on the floor writhing about and screaming for hours,” she told Sky News.
Her husband could only watch for so long before he would call an ambulance – just like he did the month prior, and the one before that.
At the hospital they would do the same checks for appendicitis, then pelvic inflammatory disease. But Amanda was sure they were looking for the wrong thing: “It’s not pelvic inflammatory disease, it’s happening every single month.”
Reports of not being believed or “gaslighting” were common among women who spoke to Sky News. One was told her pain must be a bladder infection. Two women were told it was IBS.
Nobody told Amanda it could be a failed ablation. She was the one who brought it up with her gynaecologist.
A scan revealed her womb was a “lump of scar tissue”. The only way to fix it was to remove her womb entirely.
She was shocked when her doctor told her: “Not only have I been totally misled about ablation and how amazing it is – I am now facing a major operation in order to fix it.
“If I could go back I would never have it done.
“Ablation ruined about 10 years of my life. The effect on my marriage, my work life and home life was huge.”
Taking legal action
Experiences like this are familiar to Dr Victoria Handley, a lawyer specialising in gynaecological medical negligence cases.
She estimates she’s handled about 1,000 cases relating to endometrial ablation since 2015. Every week she will hear from one or two women who have had complications from ablations.
They report adhesions of the uterus to the bladder or bowel, perforation of the uterus, infertility they weren’t warned about and ultimately needing further surgery.
Women are going to the doctor with heavy periods and ending up needing a hysterectomy, “the most radical thing you can have”, Dr Handley says. A hysterectomy carries risks including incontinence, sexual dysfunction, prolapse and early menopause.
“You’re swapping one problem for another without realising that the problem you’re swapping is actually worse than the problem you’ve got,” she told Sky News.

Dr Victoria Handley says she has handled about 1,000 cases
Exactly how many women suffer post-ablation complications is hard to pinpoint as research tends to only capture patients who have resorted to further surgery.
A study of more than 110,000 women in England who had an endometrial ablation between 2000 and 2011 found 16.7% had further surgery within five years. Other studies put the number at more than 20%.
Up to one in five ablation patients may have abnormal bleeding or period pain, or both, according to Professor Justin Clark, consultant gynaecologist and spokesperson for the Royal College of Obstetricians and Gynaecologists.
NICE guidelines set out treatment pathways for heavy bleeding. This includes taking a patient’s full history, investigating the cause of the bleeding and exploring conservative options like the coil and pill before an ablation.
A spokesperson for NHS England told Sky News staff should be following this guidance and “should make clear the benefits and potential risks of any recommended treatment so patients can make informed decisions”.
But Dr Handley says in her experience, “a lot of what’s in this guideline is ignored by the medical profession because they’ll go, ‘oh, I know what’s wrong with you’, and I’ll go straight to the surgery, and they don’t actually carry out the investigation and then send them down the correct route”.
Medical negligence cases need to establish a breach of duty; for endometrial ablation this is normally failure to warn of the risk of complications or failure to offer alternatives.
The claimant needs to prove they were injured, and the injury was caused by the breach. They also need to be able to show logically that had they been informed of the risks or alternatives, they would not have gone ahead with the ablation. If those four things don’t align, the case will fail, Dr Handley says.
The majority of cases are settled by NHS trusts out of court, she says, and women tend to receive upwards of £20,000, depending on the injury they have suffered.
Despite the number of cases she has dealt with, she says she has seen no attempt to solve the issue.
“The NHS response is woeful. There’s no joined up thinking at all. There’s no recognition that there’s an overarching problem, and there’s no desire to fix it.”
NHS England and NHS Scotland did not address questions from Sky News about how they are responding to this at an organisation-wide level.
‘It makes me sick to know my womb is burned’
Emma Burchell says she does not believe the risks were discussed in full when she had an ablation – which she calls “the worst decision I ever made”.
“You trust these doctors to do the right thing for you, and then you feel like they’ve not,” she says.
The months since the procedure in May 2022 have been “horrendous”. Constant sharp pain through her back, stomach and legs drove her to the doctor again and again, but she says she wasn’t given pain relief.
Instead she was offered antidepressants. She declined, worried she would be told the pain was “all in her head” if she accepted.
Now she’s considering a hysterectomy. “Do I need my womb?” she questions. “It makes me sick to know my womb is all burned, and it’s sat inside my stomach.”
But getting more surgery isn’t a quick fix. Gynaecological waiting lists in England have more than doubled since the start of the pandemic.
Emma has been put on injections to create a chemical menopause, a process which can help diagnose the cause of gynaecological symptoms, before doctors will consider a hysterectomy. In the meantime, each day is a “battle”.

Emma Burchell says getting an ablation was the ‘worst decision’ she’s ever made
Unsuitable candidates for ablation
A number of factors make an ablation more likely to fail: a younger age, fibroids, previous C-sections, polyps, a retroverted uterus (where the womb tips backwards) and adenomyosis (where the womb lining grows in the muscle of the womb).
According to Professor Clark, “endometrial ablation works best for women above 40 years old with relatively normal sized wombs without significant fibroids”.
Studies stress the importance of making sure women are good candidates for the procedure. A medical device alert from the UK’s Medicines and Healthcare products Regulatory Agency said the same.
Still, Sky News spoke to women who between them had all the contraindications above and had been given an ablation.
Karen Ramage found out after her ablation that she had a retroverted uterus – increasing the chance of ablation failure sixfold – as well as fibroids.
Ablations can be done where women have small fibroids, but she was told in her case it was like trying to “wallpaper over air bubbles and lumps, so it doesn’t cover the whole surface”.
When ablations work
Endometrial ablation support groups have sprung up on Facebook; the largest has more than 14,000 members, mostly in the US.
Women share stories of nerve damage, sepsis, infections, bloating, continued heavy bleeding. It’s nerve wracking reading for people considering the procedure – or who had it done before finding the group.
Samantha Williams hovers in the group, popping up in the comments to share her experience and reassure people. She had an ablation after 18 months of non-stop bleeding and it made a “massive difference” to her quality of life. It stopped the bleeding and hasn’t caused pain.
Read more on Sky News:
New workplace standards for menopause and menstruation support
Women more likely to suffer migraines during menstrual cycle
If you think of treatments for heavy bleeding as the alphabet, she says, a hysterectomy is Z. With her NHS gynaecologist they worked through until they got to Y, an ablation.
The risks were explained, the patient information leaflet was detailed and she was confident it was right for her.
Still, her advice is the same as women who had bad experiences: “Do your homework. But also try everything else first. It shouldn’t ever be the first thing that you do. There’s lots of other options.”
What the NHS says
Sky News contacted NHS England and Scotland, as well as the NHS trusts that treated Karen, Amanda and Emma.
NHS England said endometrial ablation is “one of a number of treatments” for heavy bleeding that is given “when clinically appropriate”.
“While most women do not experience significant pain after this procedure, we strongly encourage any woman with concerns to speak to their clinician or GP,” it said.
A Scottish government spokesperson said “person-centred care” was a priority and involved working in partnership with patients to understand what they need, and how their desired outcomes can be achieved.
“An essential component of this approach involves providing tailored, understandable information so that people are fully informed and involved in decision-making about their care as much as they choose.”
A spokesperson for Bolton NHS Foundation Trust said: “We welcome the opportunity to speak with any patient directly if they had concerns about their care or treatment, so we can fully understand their experience and make improvements where possible.”
NHS Forth Valley again said it followed guidelines and best practice, adding that treatment options may be discussed at multidisciplinary team meetings to identify the most suitable options.
Follow up investigations would be carried out where there is ongoing pain or other symptoms, which could identify unrelated medical conditions as the source of pain, the spokesperson said.