


In Starkville, they stormed the field with cowbells.
In Gainesville, they might soon be storming the castle with pitchforks.
For the SEC’s tale of two cities on Saturday, it was the best of times for Mississippi State and, if not the worst of times for Florida, it was perhaps the moment any hope for a revival under Billy Napier reached its nadir.
It was a Saturday about which much of the college football world offered a collective yawn in advance, but the day delivered its share of highlights and surprises, from Clemson‘s early struggles against Troy, to Baylor‘s rollicking comeback against SMU, to Bill Belichick racking up win No. 1 in college.
But all of that took second billing behind the audacity of the two most unlikely scores in the SEC.
Mississippi State, which had been in danger of being relegated to the title of “new Vandy,” had won just one of its past 17 games against Power 4 competition, but when No. 12 Arizona State rolled into Starkville on Saturday, the Bulldogs were ready.
Quarterback Blake Shapen threw touchdown passes of 48 and 47 yards and, with 30 seconds remaining in the game and trailing by 3, a 58-yarder to Brenen Thompson to seal the 24-20 win.
0:40
Mississippi State upsets Arizona State on game-winning TD
Blake Shapen throws the game-winning touchdown in the final minute as Mississippi State upsets Arizona State.
What followed was utter euphoria unseen in Starkville since they announced the opening of a new Bass Pro Shops. The fans stormed the field, pulled down the goalposts, and, we assume, carried them off to be displayed at the town’s most sacred shrine: the Chili’s off Route 12.
– no context college football (@nocontextcfb) September 7, 2025
Meanwhile, after USF’s go-ahead field goal as time expired knocked off the 13th-ranked Gators 18-16, Florida fans were left to rage against the football gods at their town’s most sacred shrine: the Chili’s off Archer Road.
Last season’s late run that included wins over LSU, Ole Miss and Florida State had offered ample hope that, perhaps, things were finally turning for the Gators. The post-Tim Tebow era has had its highlights, but each was followed almost immediately by a sudden, sharp and occasionally such massive failure that it could only be described as “Zook-tastic.” And so it was with the hope engendered by last year’s four-game winning streak, too.
DJ Lagway struggled to push the ball downfield, Florida was 4-of-12 on third down and the Gators’ defense had no answers for the magic of USF quarterback Byrum Brown, who threw for 263 yards and ran for 66 more.
When the dust settled, Napier was forced to take a hard look in the mirror and ask: “Does anyone remember my LinkedIn password?”
After watching the USF-Florida game, the Department of Labor Statistics has revised Friday’s jobs report from the US adding 22,000 to 22,001 jobs.
– ����️♈️�� (@ADavidHaleJoint) September 6, 2025
Florida still has eight games left against ranked teams, including five of its next six. The lone exception in that run is Mississippi State, which certainly doesn’t look like an easy win now either. A reality in which the Gators finish 2-10 seems entirely possible. Also, the state of Florida hasn’t had a power team finish 2-10 for, like … months.
That Mississippi State, the worst team in the SEC a year ago, could knock off last year’s Big 12 champion would normally be cause for Greg Sankey to drive his car through Brett Yormark’s rose garden while leaning out the window yelling, “Scoreboard!”
That Florida lost to an in-state team from a Group of 6 conference that doesn’t even have its own stadium would be cause for everyone who abhors the SEC’s arrogance to point and laugh and let the air out of Kirby Smart’s tires.
That both occurred on the same Saturday, within hours of each other, is destined to leave us all feeling a bit unfulfilled. Two weeks into a new college football season, perhaps that’s a good thing. That even the mighty SEC feels so uncertain is a reminder that we’ve just begun this story. We don’t yet know who the heroes are, which makes it entirely possible Mississippi State will be one. We don’t yet know which characters will meet with a tragic end, though Napier and Virginia Tech‘s Brent Pry certainly look the part.
If these are the opening chapters of 2025’s Dickens novel, we’re in for a heck of a ride the rest of the way.
Jump to a section:
Trends | Rivalries | Under the radar
Heisman five | Notes from the road
Week 2 Vibe Check
Each week, the biggest games grab the headlines, but dozens of other performances move the needle in college football, too. We try to capture those here.
Trending up: Illinois’ tournament hopes
Duke outgained Illinois by 19 yards on Saturday but still managed to lose by 26 points, 45-19. It was a nifty statistical trick that can be blamed on a flurry of takeaways by the Illini defense, which converted four Duke fumbles and a Darian Mensah interception into 21 points. After the game, Duke noted the strangeness of the outcome, pointing out that it usually waits until the Elite Eight to waste a strong offensive performance because of too many turnovers.
Trending up: Stern discipline
Syracuse narrowly escaped an upset bid against UConn on Saturday, 27-20 in overtime. Syracuse trailed 14-3 at one point, took a 20-17 lead into the final minute of action, then saw the Huskies tie the game with a 41-yard field goal as time expired. A defensive stand in overtime preserved the win, but head coach Fran Brown was less than pleased with the overall performance, forcing his players to run sprints after the game.
You can tell Fran Brown is not happy after that game. He’s making the entire team run sprints post game right now.@NunesMagician pic.twitter.com/lnNl0U6ULy
– Christian De Guzman (@CTDeGuz) September 6, 2025
Worse, Brown also gave explicit “no iPad for a week” orders and put QB Steve Angeli in timeout until he calmed down.
Trending down: Ill-fitting jerseys
Against Gardner Webb, Georgia Tech nearly repeated the brutal start it endured a week earlier vs. Colorado. In Week 1, the Jackets turned over the ball on each of their first three drives. This time, they fumbled away their first possession and tossed a pick on the next. Tech did rebound nicely for a 59-12 win, but the real disappointment was the lack of the Snuggy Jersey (the jersey roomy enough for the whole family to snuggle up and watch old footage of Paul Johnson’s offense, but versatile enough to wear when returning kicks). Unfortunately, Tech head coach Brent Key was not a fan and banished the jersey for good. It’s now stored in College Football’s forgotten treasures warehouse next to the Turnover Chain, Civil ConFliCt trophy and Houston Nutt.
I need to know more about why the Georgia Tech Punter has a XXL Jersey. Did he forget his? Switch numbers ?? There has to be a good reason for it.
�� pic.twitter.com/tkib90Lxno– Alison Mastrangelo (@AlisonWSB) August 30, 2025
Trending up: Celebrity showdowns
There was plenty of star power on display in Boulder, Colorado, in Week 2 as the Buffaloes welcomed Delaware. On one sideline was Deion Sanders, an NFL Hall of Famer, former two-sport star, reality TV personality and one of the biggest brands in sports. On the other sideline was Delaware, which is the country’s fifth-largest producer of shoehorns. The paparazzi was out in full force hoping to get a shot of Coach Prime or Delaware’s Ryan “Coach Tac-Shaver Infomercial on the CW at 3 a.m.” Carty, but the edge, in the case, went to Sanders. His Buffs overcame a sluggish start, no doubt due to being in awe of all the celebrities on Delaware’s sideline (Judge Reinhold, Teri Polo, the guy who works the overnight shift at the Wawa on Union Street), winning 31-7 behind two touchdown passes from third-string QB Ryan Staub. The Hens, meanwhile, had to settle for drowning sorrows with other A-listers at Elisabeth Shue’s late-night hot tub party.
Trending up: Revenge games
If last week was Florida State‘s coming-out party in a win over Alabama, Week 2 offered the Seminoles a chance to enjoy some sweet revenge. FSU walloped East Texas A&M 77-3, then celebrated by shouting, “That’s what you get for stealing Jimbo Fisher” and “We just scored a point for every $1 million you had to pay him to leave” all while its battered opponents helplessly insisted that, in fact, East Texas A&M is a completely different school than Texas A&M.
Trending up: Participation trophies
Division III Rowan was up 17-14 against Case Western with 2:07 left in the third quarter Saturday when a spate of bad weather rolled through — stand by, we’re Googling “Where is Rowan?” — New Jersey, suspending the action. Both sides waited patiently for four hours, listening, we assume, to Bruce Springsteen’s “The River” album on repeat, before school officials, coaches and the referees mutually agreed, according to Rowan’s press release, to call the game a 17-17 tie. The last tie at the FBS level of college football came 30 years ago when a Wisconsin and Illinois game finished 3-3, leading to the advent of overtime throughout college football and the forward pass in the Big Ten.
Trending up: Cash cows
Earlier in the week, Oklahoma State coach Mike Gundy lamented all the money Oregon spent to build a winner, only for Ducks coach Dan Lanning to retort with a series of “Yo momma’s so poor” jokes and a 69-3 drubbing of the Pokes on Saturday. Meanwhile, Oklahoma, flush with enough cash this offseason to lure star transfers such as QB John Mateer, held off Michigan, a school whose NIL budget is currently earmarked to pay down NCAA fines and get Connor Stalions that new telescope and fake beard he has been asking for, 24-13. The lesson: Teams are only as good as their players, and good players don’t come cheap. On a totally unrelated note, we just received an email from a deposed oil baron in Oklahoma who just needs our credit card and social security numbers to help secure a fortune, which he’ll happily share with us.
Trending down: Coaching legacies
On Nov. 17, 2007, Nick Saban’s Alabama team lost to Louisiana-Monroe 21-14. On Saturday, Kalen DeBoer’s Alabama team beat Louisiana-Monroe 73-0. The math on this is pretty simple: DeBoer is approximately 10 times as good a coach as Saban.
Meanwhile, Clay Helton made his long-awaited return to Los Angeles, taking his Georgia Southern team to USC, a school that fired him in 2021 despite a .657 win percentage at the school — right in line with the Trojans’ current coach, Lincoln Riley (.651). But on Saturday, Riley and USC rolled to a 59-20 win, proving once and for all that hiring him was absolutely the right call.
Rivalry Rundown
Week 2 isn’t a true rivalry week, but it did feature a number of passionate tilts between old enemies.
Cy-Hawk Trophy
Iowa State defeated Iowa 16-13 and held on to the Cy-Hawk Trophy thanks to a pair of circus catches by tight end Gabe Burkle on a go-ahead fourth-quarter drive.
WHAT. A. GRAB.
Gabe Burkle & the Cyclones are in Iowa territory with 2 minutes left pic.twitter.com/J77SRMFfu2
– Bussin’ With The Boys (@BussinWTB) September 6, 2025
It’s the sixth time in the past seven years of the rivalry in which neither team topped 20 points, and in this year’s incarnation, neither squad managed more than 238 yards of offense.
Iowa State prevailed thanks to the leg of kicker Kyle Konrardy, who booted field goals of 44 yards and 27 yards, as well as a 54-yard game winner.
Iowa threw for 83 yards in the game, a tally Kirk Ferentz frustratingly noted was almost the full length of the field and should’ve been plenty enough to win. Still, as punishment, only the defense and punters were allowed to get ice cream at the Tastee-Freez afterward.
In the past seven games in this series, Iowa’s QBs have combined to complete just 51% of their throws, averaged 4.4 yards per pass, thrown just one touchdown and five picks.
Border Showdown
The hatred between Kansas and Missouri dates back nearly two centuries. The hatred between Kansas and Missouri dates back nearly two centuries, ignited by years of guerrilla warfare during the Civil War and reaching its apex when Chase Daniel engineered a truly epic series of prank calls to Mark Mangino’s house in 2007. But since 2011, when Missouri departed for the SEC, the rivalry had remained dormant — until Saturday.
The renewed ferocity between the two programs was on display early, as Kansas jumped out to a 21-6 lead, only to see Missouri roar back. Beau Pribula threw for three touchdowns in helping the Tigers pull away to a 42-31 win — their fifth straight in the series.
And, as is the customary stakes for the loser of this rivalry, Kansas is now forced to take responsibility for the Kansas City Royals.
Baylor-SMU
What was once a heated rivalry in the old Southwest Conference had gone dormant for the past nine years, but Baylor and SMU renewed hostilities in Dallas on Saturday.
SMU hadn’t won in this series since 1986 — the year before the program received the dreaded “death penalty” for running the country’s best NIL collective — but the Mustangs appeared poised to break the streak, nursing a 14-point lead with less than six minutes to play.
But Baylor didn’t back down, riding QB Sawyer Robertson to two late touchdowns to force overtime, where the Bears won on a walk-off field goal, 48-45. Robertson finished with 440 yards passing and four touchdown throws, then did doughnuts in SMU’s parking lot in a Trans Am with a big gold eagle on the hood, just for spite.
Bayou Bucket Classic
Houston upended in-city rival Rice 35-9 behind 132 yards rushing and two touchdowns from running back Dean Connors. The win means, for the second straight year, Houston retains the Bayou Bucket. But don’t feel bad, Rice. Popeye’s sells a Bayou Bucket with three sides for just $21.99. You really can’t beat that deal.
Under-the-radar play of the week
With five minutes left in the first half, and Kent State already trailing 38-0, center Dustyn Morell delivered a play that perfectly sums up the current state of the Golden Flashes program.
Worst snap in football history
Thank you Kent State pic.twitter.com/tgZ85ATr2Y
– Unnecessary Roughness (@UnnecRoughness) September 6, 2025
Texas Tech scored following the fumble recovery and went on to win 62-14. It’s hard to entirely fault Morell though. He’d been eating caramels before the play and his hands were sticky.
Under-the-radar game of the week
With just 1:43 to go, UMass allowed Bryant — a team that’s just 11 guys who all showed up at the local YMCA wearing Kobe Bryant jerseys on the same day — to march 78 yards and drill a 25-yard game-winning field goal. The Minutemen fell 27-26, the most embarrassing moment in the program’s football history since — we’re guessing last week. The good news for UMass is it’s just a mere 35 days away from playing Kent State.
Heisman five
Arch Manning is currently sitting in his car outside the Heisman House listening to mix tapes and wondering how many touchdown passes a guy has to throw against San Jose State to earn a guest pass for the weekend.
1. Oklahoma QB John Mateer
Against one of the nation’s best defenses, Mateer accounted for 344 total yards and three touchdowns in an Oklahoma win over Michigan, shocking fans throughout Columbus, Ohio, who had no idea such a thing was possible.
2. Utah QB Devon Dampier
After torching UCLA in its opener, Utah beat Cal Poly with ease Saturday, as Dampier accounted for three touchdowns for the second straight week. Unfortunately, because the game happened in Utah, no Heisman voters watched.
3. Florida State QB Tommy Castellanos
One week after running all over Alabama, Castellanos used his arm to torch East Texas A&M, racking up 237 yards and three touchdowns. Normally, the ultraconfident Castellanos would talk a little smack to next week’s opponent to set the stage, but FSU gets Kent State in Week 3 and, honestly, that probably doesn’t feel worth it.
4. Baylor QB Sawyer Robertson
Robertson has thrown for 859 yards and seven touchdowns without a pick through two games — both against upper-tier Power 4 competition. He’s suddenly turning heads among NFL scouts. Also, the drive-thru girl at Whataburger threw in some extra fries the last time he was there.
5. LSU QB Garrett Nussmeier
Nussmeier had a less-than-exciting performance in a 23-7 win over Louisiana Tech, throwing for 237 yards, one touchdown and a pick. It was part of a trend of SEC teams struggling to put away lesser competition Saturday, as Georgia and Texas A&M also waited until late in the second half to secure their wins. At least they’re all not Florida.
Game day notes
![]()
![]()
In making repeated comments about the disparity between Oregon’s budget and Oklahoma State’s earlier this week, head coach Mike Gundy might have both preempted and prompted what transpired at Autzen Stadium on Saturday.
From kickoff, the Ducks dominated every phase of the game on their way to a commanding 69-3 shellacking of the Cowboys. The way Oregon came out of the gates, stepped on the gas pedal and didn’t take their foot off until they were up 48-3 halfway through the third quarter when they brought in the offensive backups (who still got a touchdown of their own) seemed very purposeful. Not only did the Ducks seem interested in beating Gundy’s team, but also in making a statement.
Oregon did not punt until the fourth quarter (their first punt of the season in two games), and the only drive it had through its first eight that did not end in a score was a turnover on downs in the first quarter. The Ducks had a 59-yard touchdown run on their second offensive play of the game and a 65-yard touchdown pass on their third offensive play of the game. Explosive plays were everywhere at Autzen as the OK State defense provided little to no resistance on the day.
The back-to-back pick-sixes late in the third quarter to take the score of the game from simply overwhelming to outright historic were just salt on the wound. As teams exited the field once the clock hit zero, AC/DC’s “Moneytalks” played over the speakers, fittingly serenading Oklahoma State on its way back to Stillwater.
For the Pokes, it was the kind of performance that might prompt a deeper look at the state of their program. For the Ducks, it was a showcase that showed why, despite losing their starting quarterback, top receiver and elite linemen on both sides of the ball after last season, Oregon still has the depth and talent to be a title contender. — Paolo Uggetti
![]()
![]()
When Beau Pribula made what he called “an impossible decision” in December to leave Penn State as the Nittany Lions were preparing for the College Football Playoff, he did so to set himself up for days such as Saturday. Pribula left Happy Valley for the opportunity to compete for a starting job elsewhere, quickly landing at Missouri, where starter Brady Cook was out of eligibility.
Coming out of training camp, Mizzou coach Eli Drinkwitz said the quarterback competition between Sam Horn and Pribula would extend into the season, but Pribula inherited the job by default when Horn was injured on his first snap last week. Pribula shined in that game against FCS Central Arkansas, but considering the level of competition, it was hard to read too much into his performance. This week, it was different. With the rivalry against Kansas renewed, Pribula completed 30 of 39 passes for 334 yards with three touchdowns and no interceptions in the 42-31 win. He looked the part of a quarterback who can successfully lead the Tigers into the SEC gauntlet that awaits.
Considering the circumstances of his departure from Penn State, Pribula’s immediate success must come with an extra layer of satisfaction for him. He would have been stuck behind Drew Allar again at Penn State and now has shown the country he, too, can play at a high level. Pribula’s situation in December was a factor in the recent proposal by the FBS Oversight Committee to move the transfer portal window to January, so it will have less overlap with the playoff. — Kyle Bonagura
![]()
![]()
Exhale, Horns, Arch is all right. A week after a disappointing performance in a 14-7 loss at Ohio State, Arch Manning got off to a bit of a slow start again on a sleepy, overcast, 11 a.m. Austin kickoff. He started 3-of-6 for 11 yards on the Longhorns’ first two drives, including a badly overthrown ball to Ryan Wingo that could’ve been intercepted if the defender had another step.
But on the next drive on third down, Manning got an easy throw and catch to Parker Livingstone, who turned it upfield as a defender slipped and raced 83 yards for a touchdown. By halftime, Manning was on fire and the rout was on, including three straight touchdown passes on three straight attempts, as Texas scored four touchdowns in 4:56 of game time.
But it wasn’t all smooth for Manning. He heaved an ill-advised throw into double coverage under pressure for an interception at the San Jose 13. He fumbled on a sack at his own 1-yard line in the third quarter but recovered it.
But he came back with a 20-yard touchdown run, tiptoeing down the sideline and showcasing the athletic ability that coach Steve Sarkisian said this week he should embrace.
The Longhorns had too many penalties (12-115), a few dropped passes and some protection problems they’ll need to get fixed before SEC play starts. But the defense held the Spartans in check, forced four turnovers a week after not having one against the Buckeyes, and Manning joined Colt McCoy, Vince Young and David Ash as the only Texas QBs over the past 20 years with two or more games of two 20-plus-yard TD passes and a 20-plus-yard TD run.
Sarkisian said he was pleased with the response by a quarterback who could’ve let his competitiveness linger after last week’s disappointment.
“I think he’s hard on himself differently than maybe I’m hard on him, but I’m also trying to ease some of that,” Sarkisian said. “When he gets hard on himself, I try to back himself off of that and try to make sure he’s got the right amount of confidence when he goes and plays because he’s a very talented player.” — Dave Wilson
![]()
![]()
Illinois eventually resembled a College Football Playoff contender at Duke, but first it reinforced the importance of being opportunistic and finding new ways to win. The Illini were sluggish in the first quarter and for much of the first half. Their celebrated offensive line couldn’t keep Vincent Anthony Jr. and Duke’s pass rushers away from quarterback Luke Altmyer. A Bret Bielema-coached team surprisingly couldn’t run the ball. At times, Illinois didn’t really look ready.
But the Illini found themselves on the right side of the handful of plays that determine outcomes. Duke’s repeated mistakes on special teams and on offense in Illinois’ end of the field were too many to overcome. Any team that is minus-5 in turnovers on its home field has no business winning.
Still, Illinois had to capitalize and did behind Altmyer, whose experience and talent showed up repeatedly. Altmyer completed 22 of 31 passes for 296 yards and three touchdowns with no interceptions, spreading the ball to a largely new group of wide receivers. Illinois certainly misses Pat Bryant and Zakhari Franklin, but offensive coordinator Barry Lunney Jr. hoped for more explosiveness with this receiving corps and got it, as Hank Beatty, Justin Bowick and others delivered.
Bielema’s championship teams at Wisconsin were built on elite line play and the power run. This Illini squad hasn’t really hit its stride with the run game, and ultimately might be pass-heavy with one of the nation’s more proven quarterbacks in Altmyer and a dynamic group of wideouts. Illinois won’t be able to count on every opponent to make the number of mistakes Duke did, but the Illini now have a track record of taking advantage, which should serve them well during Big Ten play. — Adam Rittenberg
![]()
![]()
The curse is broken. Matt Campbell and his Cyclones have finally defeated Iowa in Ames for the first time in his tenure. Iowa State’s latest bout with its rival, a 16-13 win, was a nail-biter decided in the final minute as usual.
In securing its first home win over Iowa since 2011, Iowa State has won three of its past four against its in-state foe. Six of the past seven Cy-Hawk winners have scored 20 points or less. It takes a remarkable amount of toughness to survive these low-scoring brawls.
But this might be Campbell’s toughest team yet.
Throughout his tenure, the head coach has fixated on “winning on the margins,” doing all the little things right to overcome any talent deficit and get games into the fourth quarter. These days, the proof is in the results: Iowa State has won eight of its past nine games decided by one-score margins.
Kicker Kyle Konrardy got to be the Cy-Hawk hero yet again, drilling a clutch 54-yard go-ahead field goal in the final two minutes. He got that opportunity thanks to Rocco Becht guiding a 13-play, six-minute drive in the fourth quarter that featured three third-down conversions. Iowa State’s defense finished the job with pass rusher Tamatoa McDonough, a little-known transfer from Yale, slamming Iowa quarterback Mark Gronowski down for back-to-back sacks to kill any hopes of a game-winning drive.
“These are milestone moments,” Campbell said. “Our kids, the schedule, what we’ve been up against — real toughness.”
This team had to have the right stuff from the start to pull this off. It took everything the Cyclones had to survive a 24-21 win over Kansas State in Ireland during Week 0. Then they had to come home and figure out how to keep playing their best ball. In many ways, they still haven’t. But what Campbell loves most is the way this Becht-led squad plays with steady resolve, how it can hang in there when things aren’t going its way and keep pushing.
This rivalry win is more proof that this group knows how to win in the fourth quarter — and the Cyclones might be ready to go win the Big 12, too. — Max Olson
UK
890 people arrested at Palestine Action protest yesterday – including 17 on suspicion of assaulting police officers


The Metropolitan Police has said 890 people were arrested at a protest against the banning of Palestine Action as a terror group on Saturday – including 17 on suspicion of assaulting officers.
A total of 857 individuals were arrested in Parliament Square in London under the Terrorism Act 2000 over alleged offences, the force said.
It added that a further 33 were arrested for other offences, with 17 of those detained on suspicion of assaulting officers. The Met Police did not say what the other 16 arrests were for.
Deputy Assistant Commissioner Claire Smart, who led the policing operation, thanked Met Police officers for their “professionalism and tireless work despite the level of abuse that they faced”.
Pic: PA
Ms Smart said: “The violence we encountered during the operation was coordinated and carried out by a group of people, many wearing masks to conceal their identity, intent on creating as much disorder as possible.
“Many of those individuals have now been arrested and we have begun securing charges.”
Defend Our Juries, which organised the demonstrations, insisted the rally was “the picture of peaceful protest”.
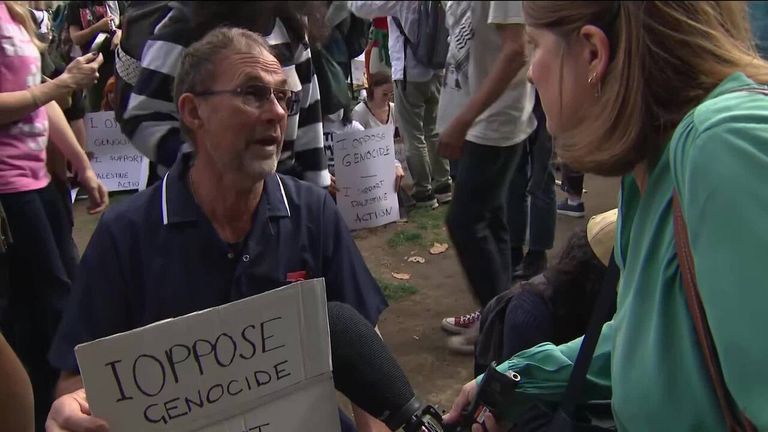
‘Do I look like a terrorist?’ nurse at protest asks Sky News
Ms Smart also claimed that the “contrast between this demonstration and the other protests we policed yesterday, including the Palestine Coalition march attended by around 20,000 people, was stark”.
She added: “You can express your support for a cause without committing an offence under the Terrorism Act or descending into violence and disorder, and many thousands of people do that in London every week.
“We have a duty to enforce the law without fear or favour. If you advertise that you are intending to commit a crime, we have no option but to respond accordingly.”
Defend Our Juries previously estimated 1,500 had gathered for the rally on Saturday, where many held signs saying: “I oppose genocide. I support Palestine Action.”

Pic: PA

Pics: PA
The group has been banned as a terror group since 5 July after MPs voted overwhelmingly in favour of the move proposed by then-home secretary Yvette Cooper, making it illegal to express support for the group.
It came shortly after two Voyager aircraft suffered around £7m worth of damage at RAF Brize Norton in Oxfordshire on 20 June.
Defence Secretary John Healey told Sky’s Sunday Morning With Trevor Phillips that he expects newly appointed Home Secretary Shabana Mahmood to be “just as tough” as her predecessor on Palestine Action.
He said: “I expect her to defend the decision the government has taken to proscribe Palestine Action because of what some of its members are responsible for, and were planning for.”
Read more from Sky News:
Israel warns Gaza City residents to flee
Anger over Israeli president’s planned visit to UK
Sydney beaches closed after fatal shark attack
The Met Police previously said the consequences for those charged under the Terrorism Act include a maximum sentence of six months’ imprisonment.
The Home Office is set to appeal against the High Court ruling allowing Palestine Action’s co-founder, Huda Ammori, to proceed with a legal challenge against the government over the group’s ban.


Defence Secretary John Healey has told Sky News the government is considering using military barracks to house asylum seekers, as an estimated 1,000 people arrived in the UK on small boats on Saturday.
“We are looking at the potential use of military and non-military sites for temporary accommodation for the people who come across on these small boats that may not have a right to be here,” he told Sunday Morning With Trevor Phillips.
“I’m looking really hard at it. I’m looking at it with the Home Office, and I recognise that the loss of confidence of the public over recent years in Britain’s ability to control its borders needs to be satisfied. And we have to deal with this problem with the small boats,” Mr Healey added.
Politics latest: Labour considers housing migrants on military sites
The measure follows widespread protests this summer over housing migrants in hotels.
Fresh small boat arrivals were spotted on Sunday, after an estimated 1,000 people arrived on Saturday – when French authorities said 24 people were rescued while trying to cross the Channel.
The figures compare to a relatively recent lull in crossings. In the previous seven days (30 August to 5 September) the Home Office recorded no small boat arrivals.
Zia Yusuf, head of policy at Reform UK, told Trevor Phillips that Britain has become a “soft touch” on migration, before suggesting between 15 and 25 detention sites will need to be built to detain asylum seekers. He described these as “purpose-built modular steel structures”.
“We can look around the world at where things have worked and worked well. President Trump stood up 3,000 detention beds in eight days. That was this year in the state of Florida – using steel modular structures,” Mr Yusuf said.
He added that the president’s crackdown has significantly reduced illegal border crossings and suggested the same could happen in the English Channel to deter migrants.
“These are unarmed, largely men in dinghies, we don’t need a particularly formidable military to be able to take them to a detention centre,” he said.
Zia Yusuf from Reform UK said he believes Britain has become a “soft touch” on migration
Shabana Mahmood will have the job of tackling illegal immigration after taking over from Yvette Cooper as home secretary on Friday – when Sir Keir Starmer carried out a major cabinet reshuffle following the resignation of his deputy prime minister Angela Rayner.
National Crime Agency (NCA) figures show record levels of disruption of immigration crime networks in 2024/25.
Join the Sky News immigration debate
Officials believe this contributed to the lowest number of boats crossing the Channel in August since 2019.
But, despite the 3,567 arrivals in August being the lowest since 2021, when looking across the whole of 2025, the figure of 29,003 is the highest on record for this point in a year.
Sky’s Political Correspondent Liz Bates said that after Labour scrapped the previous government’s controversial Rwanda policy and shut down the Bibby Stockholm barge, ministers are “hitting up against many of the same problems” with “a really broken and very slow asylum system”.
“The context to all of this is a huge shake-up at the Home Office, and I think something of an admission that [Yvette] Cooper, despite her years of experience, could not get a grip… of this problem of people coming across the Channel in small boats and then ending up in asylum hotels,” she added.
Army bases were previously used by the Conservative government, but this prompted local protests, and the sites were widely criticised for their poor conditions in some cases.
Read more from Sky News:
Farage wants Afghan women deported
Huge rise in asylum protests
Attack on Epping asylum seeker
As Sky’s Home Editor Jason Farrell writes, Ms Mahmood has become the home secretary of a country where the national flag is being hoisted as a symbol of dissatisfaction – with anger at the arrival of desperate migrants crossing the Channel in small boats.
Sir Keir’s sweeping changes
Sir Keir Starmer has announced sweeping changes to his ministerial team in the Home Office as his government works to get a grip of illegal migration to the UK.
Here’s a list of who has been moved, besides the home secretary.
Dame Angela Eagle, who was border security and asylum minister, has been moved to the environment department.
Dame Diana Johnson, who was policing and crime minister, has been moved to the Department for Work and Pensions (DWP).
She has said in a post on X that it was an “honour” to work with police officers, and she is “delighted” to be moving to the DWP.
Dan Jarvis has been given a role in the Cabinet Office, in addition to his post as security minister in the Home Office.
And Sarah Jones, who was industry minister, has been moved to the Home Office.
-
 Sports3 years ago
Sports3 years ago‘Storybook stuff’: Inside the night Bryce Harper sent the Phillies to the World Series
-
 Sports1 year ago
Sports1 year agoStory injured on diving stop, exits Red Sox game
-
 Sports2 years ago
Sports2 years agoGame 1 of WS least-watched in recorded history
-
 Sports2 years ago
Sports2 years agoMLB Rank 2023: Ranking baseball’s top 100 players
-
 Sports2 years ago
Sports2 years agoButton battles heat exhaustion in NASCAR debut
-
Sports4 years ago
Team Europe easily wins 4th straight Laver Cup
-
 Environment2 years ago
Environment2 years agoJapan and South Korea have a lot at stake in a free and open South China Sea
-
 Environment11 months ago
Environment11 months agoHere are the best electric bikes you can buy at every price level in October 2024