

Spring statement: Rachel Reeves can make decisions on spending cuts without too much fallout for now – but worse could be yet to come
Rachel Reeves will keep her remarks short when she delivers the spring statement on Wednesday.
But the enormity of what she is saying will be lost on no one as the chancellor sets out the grim reality of the country’s finances.
Her economic update to the House of Commons will reveal a deteriorating economic outlook and rising borrowing costs, which has forced her to find spending cuts, which she’s left others to carry the can for (more on that in a bit).
Politics Live: Polling suggests almost everyone is pessimistic
The independent Office of Budget Responsibility (OBR) is expected to forecast that growth for 2025 has halved from 2% to 1%.
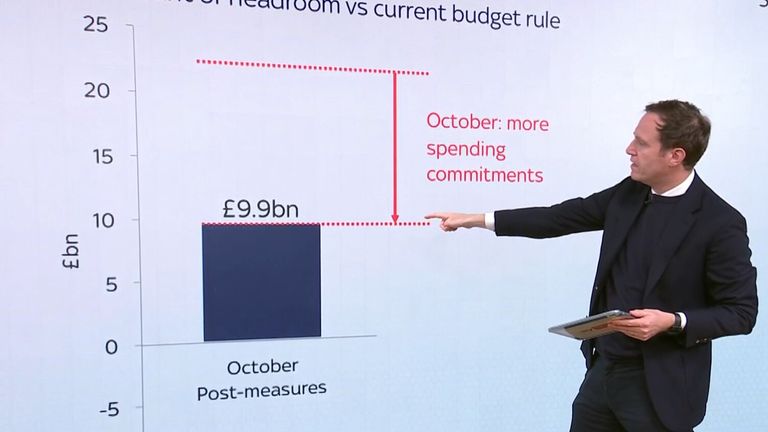
That, combined with rising debt repayment costs on government borrowing, has left the chancellor with a black hole in the public finances against the forecasts published at the budget in October.
Back then, Reeves had a £9.9bn cushion against her “iron-clad” fiscal rule that day-to-day spending must be funded through tax receipts not debt by 2029-30.
But that surplus has been wiped out in the ensuing six months – now she finds herself about £4bn in the red, according to those familiar with the forecasts.
That’s really uncomfortable for a chancellor who just months ago executed the biggest tax and spend budget in a generation with the promise that she would get the economy growing again.
At the first progress check, she looks to be failing and has been forced into finding spending cuts to make up the shortfall after ruling out her other two options – further tax rises or more borrowing via a loosening of her self-imposed fiscal rules.
What to expect in the spring statement
‘World has changed’
When Reeves gets up on Wednesday, she will put it differently, saying the “world has changed” and all that means is the government must move “further and faster” to deliver the reforms that will drive growth.
But her opponents will be quick to lay economic woes at her door, arguing that the unexpected £25bn tax hike on employers’ national insurance contributions last October have choked off growth.
But it’s not just opposition from the Conservative benches that the chancellor is facing – it is opposition from within as she sets about cutting government spending to the tune of £15bn to fill that black hole.
Politically, her allies know how awkward it would have been for the chancellor to announce £5bn in welfare cuts to avoid breaking her own fiscal rules, with one acknowledging that those cuts had to be kept separate from the spring statement.
There’s also expected to be more than £5bn of extra cuts from public spending in the forecast period, which could see departments that don’t have protected budgets – education, justice, home – face real-term spending cuts by the end of the decade.

Pic: PA
Not an emergency budget
We won’t see the detail of that until the Spending Review in June.
This is not an emergency budget because the chancellor isn’t embarking on a round of tax raising to fix the public finances.
But these are, however they are framed, emergency spending cuts designed to plug her black hole and that is politically difficult for a government that has promised no return to austerity if some parts of the public sector face deep cuts to stick with fiscal rules.
If that’s the macro picture, what about the “everyday economics” of peoples’ lives?
I’d point out two things here. On Wednesday, we will get to see where those £5bn of welfare cuts will fall as the government publishes the impact assessment that it held back last week.
Read more:
Corbyn brands benefit cuts a ‘disgrace’
Expect different focus from Reeves at spring statement
Up to a million people could be affected by cuts, and the reality of who will be hit will pile on the pressure for Labour MPs already uncomfortable with cuts to health and disability benefits.

Benefits cuts explained
The second point is whether the government remains on course to deliver its key pledge to “put more money in the pockets of working people” during this parliament after the Joseph Rowntree Foundation think-tank produced analysis over the weekend saying living standards for all UK families are set to fall by 2030.
The chancellor told my colleague Trevor Phillips on Sunday that she “rejects” the analysis that the average family could be £1,400 worse off by 2030.
But that doesn’t mean that the forecasts published on Wednesday calculating real household disposable income per head won’t make for grim reading as the economic outlook deteriorates.
Nervousness in Labour
Ask around the party, and there is obvious nervousness about how this might land, with a degree of anxiety about the economic outlook and what that has in store for departmental budgets.
But there is recognition too from many MPs that the government has political space afforded by that whopping majority, to make these decisions on spending cuts without too much fallout – for now.
Because while Wednesday will be bad, worse could be yet to come.
Staring down the barrel
The chancellor is staring down the barrel of a possible global trade war that will only serve to create more economic uncertainty, even if the UK is spared from the worst tariffs by President Donald Trump.
The national insurance hike is also set to kick in next month, with employers across the piece sounding the warnings around investment, jobs and growth.
Six months ago, Reeves said she wouldn’t be coming back for more after she announced £40bn in tax rises in that massive first budget.
Six months on she is coming back for more, this time in the form of spending cuts. And in six months’ time, she may well have to come back for more in the form of tax rises or deeper cuts.
The spring statement was meant to be a run-of-the-mill economic update, but it has morphed into much more.
The chancellor now has to make the hard sell from a very hard place, that could soon become even tougher still.


Bishop Ceirion Dewar rejects the Church of England as heretics. Instead, he gathers his flock under a gloomy sky on a beach in Cornwall.
More than 20 people answered the call he made on social media – one wears a T-shirt saying Jesus is King.
Another wears a Union Jack anorak with a T-shirt emblazoned “UTK” – Unite the Kingdom – the movement organised by anti-Islam campaigner Tommy Robinson.
Wearing a white robe over a wetsuit, Dewar strides down the beach and prepares for a mass baptism.
His voice booms out: “In the name of Jesus Christ, I gladly baptise you!”
Critics call Dewar “the far-right bishop” – a label he rejects.
But he does represent a new type of Christianity – more militant, more political – and one that is on the rise.
Several of those here came because they saw Dewar preaching fire and brimstone at Robinson’s Unite the Kingdom march on 13 September.
And they are ready to follow him into the cold waters of the Celtic Sea. One by one, he blesses them, then plunges them under the waves. Afterwards, they hug. Some are euphoric.

Bishop Ceirion Dewar performs a mass baptism in Bude
Fergus Worrall drove from Bristol with his girlfriend Louise French; both were baptised.
“I saw Ceirion’s speech at the Unite the Kingdom rally, and it was just epic,” Worrall says. “I mean, I just loved it.”
Worrall says he used to be “fairly lefty”. After trying Buddhism and New Age practices, he came to Christianity. But Dewar’s appeal is not just religious – online he decries immigration and the influence of Islam, a message that “chimed”.
“We are a Christian culture, a Christian nation. And I do feel like we have lost a lot of that.”
A month earlier, Dewar had addressed the 150,000-strong crowd at the Unite the Kingdom march in London, bishop’s crook in hand, his voice thundering out over Westminster: “God, you have not abandoned Britain!”
When he looked out, he saw not just British and English flags, but wooden crosses and depictions of Jesus.
It was not his first appearance with Robinson. The year before, he spoke at another rally in Whitehall and said: “This nation of ours is under attack! We are at war! We are at war not just with the Muslim, not just with wokeness.”

People stand with crucifixes at the Unite the Kingdom rally, in central London on 13 September
This is something new and growing – a movement that has long marched against immigration, against Islam, is now marching behind the cross.
I ask Dewar what for him, as a Christian, is the appeal of Robinson.
“It’s not the appeal of Tommy Robinson, per se,” he says. “It was the opportunity that he afforded to me to stand in front of that many people and to both pray for the people and this nation.”

Sky’s Data and Forensics correspondent Tom Cheshire interviews Bishop Ceirion Dewar on a beach in Cornwall
Dewar was marching front and centre with Robinson. He may be borrowing an audience from Robinson, but he’s also effectively endorsing him, I suggest – and doing so in a bishop’s garb.
“I don’t think that at all. I’m very clear on what I endorse, and my political views are public and well-founded.
“My stand with Tommy is not necessarily political. It’s a man that has surrendered his life to Christ, and he’s on that journey of faith and trying as a good shepherd to help lead him in that and to shape that faith in a way that is beneficial to him.”
I ask him whether he truly thinks we are “at war” with the Muslim.

Bishop Ceirion Dewar
“Unfortunately, what I was trying to convey, having listened to an entire day’s worth of speeches, didn’t come across quite the way I’d hoped to have expressed it,” Dewar says.
“The problem for me is I understand we’re a multi-ethnic, multicultural, multi-faith Britain, but when you have so many elements that refuse to get into the great melding pot of multiculturalism, but remain outside and try and force that culture, force that religious system, force that legal system into an existing culture, then there’s always going to be problems.
“I would love to see more Christianity at the heart of our politics. I would like to see Christian principles once again driving our legal system.”
Many on the hard and far right agree with him – and increasingly link an anti-Islam agenda with a Christian identity. That also adds grandeur to grassroots street politics, elevating a culture war into a clash of civilisations.
UKIP, which has become more explicitly nationalist since the departure of Nigel Farage as party leader, says in its manifesto that it will “declare war on radical Islam and place Christianity back into the heart of government”.
Online, people call for a “holy war”. Katie Hopkins, the far-right commentator who also marched shoulder to shoulder with Robinson, said in a recent interview: “Certainly the time of the crusades will need to come again… We are overrun.”
One group organising online, with more than 50,000 followers, uses Christian imagery as part of its pledge to “hunt down Muslims”.
Dr Maria Power, author of The Church, the Far Right, and the Claim to Christianity, describes this as “Christian nationalism” and says it has a precedent in the UK, especially in Northern Ireland, where Britishness and Christianity were often equated.
“But really, I’ve seen it increase since we’ve seen the power of Christian nationalism in the states develop. You start to see inklings of it, probably about four or five years ago. Particular pastors talking this way, podcasts emerging, and content emerging on places like YouTube. And it’s very easy to fall down the rabbit hole of the algorithm, isn’t it?”
Ceirion Dewar rejects the term Christian nationalism, which he sees as specific to the United States, a country that has a different tradition of public, political Christianity. And it’s true that he and others have been advocating and preaching a more muscular Christianity since at least 2016 and the Brexit referendum.
One of his friends is Rikki Doolan, who belongs to the Spirit Embassy, a church in London with British-Zimbabwean origins. (A 2023 investigation by Al Jazeera accused Doolan and others in the church of being involved in money laundering, an accusation Doolan describes as “fake news and a false narrative”.)
It was Doolan who “converted” Tommy Robinson to Christianity three weeks before the latter left prison earlier this year. Doolan says it is “a new journey” for Robinson.

Tommy Robinson stands at the start of the Unite The Kingdom protest in central London
Doolan was also on stage at UTK. I ask him about some of the statements made there, including by a Belgian politician, that “Islam does not belong in Europe and Islam does not belong in the UK”. He says he disagrees with that “because it’s not realistic”. But “if we can’t fix the problem, then that makes more sense. But I would like to try and fix it first”.
Doolan and Dewar stand outside the established Church. But the majority of Christians in the UK still belong to the Church of England.
Dr Sam Wells is the vicar of St Martin’s-in-the-Field, a Church of England church on the corner of Trafalgar Square in London. He was holding an annual service commemorating victims of suicide when Robinson’s march came right up to the square, resulting in skirmishes with the police. Wells says his congregation was “hurt” by the Christian imagery on display.
“The gestures of the cross, the Christian symbols, are about love and understanding and peace and gentleness and they’re being thrust in people’s faces as weapons,” he says. “I think that’s very painful.”
Wells was one of the senior clergy leaders who signed an open letter denouncing Robinson’s march as a “corruption” of the Christian faith, saying the cross was being “co-opted” by the far right. Dewar in turn wrote his own letter denouncing the Anglican hierarchy for seeking “polite applause in editorial offices and political chambers”, calling on them to “repent”.
Dr Wells says Dewar’s letter is “very well expressed but I think it’s nonsense”.
“Christian values, what does that actually mean? I think it means love, joy, peace, patience, kindness, goodness. An institution or a church or a preacher has a right to be called Christian if they look like Jesus. Those marches didn’t look like Jesus to me. They looked like the kind of people who were attacking Jesus in Holy Week.
“I think they’re reading a different Bible from the one I’m reading.”
If the talk is of winning, well there are very different battlegrounds.
The cloisters versus a Cornish beach.
Dewar has several mass baptisms planned across the country; so does Doolan.
This is not just about the extreme right using Christianity for their own ends; it’s just as much some Christians using the far right to reach new audiences.
A new Christian politics, in all sorts of ways and all sorts of places, is on the march.

People hold crucifixes at the Unite The Kingdom rally in central London
The Data and Forensics team is a multi-skilled unit dedicated to providing transparent journalism from Sky News. We gather, analyse and visualise data to tell data-driven stories. We combine traditional reporting skills with advanced analysis of satellite images, social media and other open source information. Through multimedia storytelling we aim to better explain the world while also showing how our journalism is done.


The worst offending areas for uninsured driving in the UK have been revealed – as a hit-and-run victim described how he was “left for dead” with catastrophic injuries.
Every 20 minutes, someone in the UK is hit by an uninsured or hit-and-run driver, the Motor Insurers’ Bureau (MIB) said, based on claims from over 26,000 victims each year.
Every day, at least one person is so seriously injured by an uninsured or hit-and-run driver that they need life-long care and every week, at least one person is killed by an uninsured driver, according to the bureau.
Thurrock in Essex is the worst offending area for uninsured driving, according to claim data from the MIB, a non-profit organisation created to protect people from the impact of uninsured and hit-and-run drivers.
Four different postal areas in Birmingham are among the 15 hotspots highlighted by the MIB, with areas in Peterborough, Manchester, Belfast and Havering also named due to housing a large number of defendants per 1,000 residents.
Map shows worst areas for uninsured driving in UK
The 15 worst postal areas for uninsured driving
• 1. Thurrock (RM19)
• 2. Birmingham (B25)
• 3. Birmingham (B18)
• 4. Peterborough (PE1)
• 5. Sandwell (B66)
• 6. Havering (RM1)
• 7. Birmingham (B21)
• 8. Manchester (M18)
• 9. Birmingham (B35)
• 10. Belfast (BT17)
• 11. Epping Forest (IG7)
• 12. Belfast (BT13)
• 13. Buckinghamshire (HP18)
• 14. Bradford (BD7)
• 15. Luton (LU1)

One of the victims of an uninsured driver is cyclist Cahal O’Reilly, 55, who was five miles from the ferryport in Holyhead, Wales, when he was hit from behind in September 2021.
He was thrown on to the windscreen and 20m through the air until he landed on the side of the road, seriously injured.
The uninsured driver, who police estimate was driving at 70mph, fled the scene.

Mr O’Reilly suffered catastrophic injuries, including a broken neck and back. Pic: MIB
‘Left for dead’
“I was left for dead, bleeding to death on the side of the road,” Mr O’Reilly told Sky News.
“Nobody knows how long I was on the floor for. When I came to my senses, I could taste my own blood and feel the road on my cheek.”
He realised he was “pretty seriously injured” when he could not move his ankles, and lay still until help arrived.
A passing motorist, who initially thought Mr O’Reilly’s lifeless form was debris before realising it was a body, called the emergency services.
Mr O’Reilly was left with serious injuries, including a broken back and neck, shattered pelvis, smashed bone in his leg, and dislocated shoulder and required several surgeries in the days after the crash.

Police said Mr O’Reilly would be dead if he had not worn his helmet. Pic: MIB

The back tire of Mr O’Reilly’s bicycle was completely ripped apart. Pic: MIB
“I suffered a polytrauma, which is multiple horrendous injuries,” Mr O’Reilly said. “The police said if I hadn’t been wearing a helmet, I would be dead, and officers didn’t think I would make it.
“The hospital consultant told my wife that most people don’t survive the impact, the time until the ambulance arrives, and 22 hours of operations in 48 hours.”
Doctors had to use rods to reconnect Mr O’Reilly’s knee and ankle on his right leg, as the bottom of his foot “was just hanging on by skin and muscle”, and use an arterial skin graft from his left arm to help patch up the damage to his smashed leg.
Mr O’Reilly, who lives in Wandsworth, south London, also had to wear a neck brace for more than five months to stabilise his shattered neck and had to learn how to walk again, with serious setbacks on the way.

Mr O’Reilly had to learn how to walk again after extensive surgery. Pic: MIB
‘Challenging’ recovery
“My pelvis and back fused and healed very quickly, but my leg took the main force of initial impact, with bits of my leg tissue found in the headlight of the car,” Mr O’Reilly said.
Just when he started seeing some progress in the rehab for his leg, about 18 months after the crash, doctors discovered that the metal work supposed to hold the bones together was falling apart, causing a serious infection in his leg.
Mr O’Reilly required another surgery and was told that if the bone did not heal, his leg would have to be amputated.

Mr O’Reilly’s blood and tissue were found in the headlights of the driver’s car. Pic: MIB
Four years on from the horrifying crash, he was told that his bone had finally fused last month.
“If you walk past me in the street, you wouldn’t know now, but the process to get there was very difficult and psychologically quite challenging,” Mr O’Reilly said.
The former British Army major hopes he will be able to return to work as a business consultant next year.
Read more:
Victim criticises ‘appalling’ sentence for uninsured driver
Nurse describes ‘horrific’ fatal crash
He is now campaigning with the MIB to stop uninsured drivers from hitting the roads, as he wants “nobody to go through what I had to go through”.
“We have to do something in this country,” he said. “People are morally making a choice where they don’t care about their fellow citizens and fail to insure their car and make sure it is properly taxed. Something like that is a social responsibility.”

Mr O’Reilly is campaigning with the MIB to stop uninsured motorists. Pic: MIB
£1bn cost of uninsured drivers
Uninsured driving costs the government £1bn a year, including compensation for victims, emergency services, medical costs and loss of productivity.
An uninsured vehicle is seized every four minutes across the UK, with almost 120,000 seized so far this year, the MIB said.
The bureau has launched a week-long road safety initiative in collaboration with police forces across the UK, including targeted enforcement in problem areas and public education to urge people to check their insurance status.
“Our aim is to end uninsured driving, which means working closely with the police across the UK to remove dangerous vehicles from our roads,” Martin Saunders, head of enforcement at MIB, said.
“At the same time, we are ramping up our support for motorists who want to drive legally, providing them with the knowledge they need to have the right cover in place.”
-
 Sports2 years ago
Sports2 years agoStory injured on diving stop, exits Red Sox game
-
 Sports3 years ago
Sports3 years ago‘Storybook stuff’: Inside the night Bryce Harper sent the Phillies to the World Series
-
 Sports2 years ago
Sports2 years agoGame 1 of WS least-watched in recorded history
-
 Sports3 years ago
Sports3 years agoButton battles heat exhaustion in NASCAR debut
-
 Sports3 years ago
Sports3 years agoMLB Rank 2023: Ranking baseball’s top 100 players
-
Sports4 years ago
Team Europe easily wins 4th straight Laver Cup
-
 Environment2 years ago
Environment2 years agoJapan and South Korea have a lot at stake in a free and open South China Sea
-
 Environment1 year ago
Environment1 year agoHere are the best electric bikes you can buy at every price level in October 2024