

90-second treatment for heavy periods leaves some women in agony – and needing a hysterectomy

Thousands of women every year have an endometrial ablation on the NHS.
It’s a treatment for heavy periods – and for a lot of women, the 90-second procedure brings relief from the sapping cycle of heavy bleeding.
But the procedure to destroy the womb lining fails in up to a fifth of cases, often leaving women with no treatment options left but a hysterectomy.
People whose ablations have failed describe debilitating, long-lasting pain that fractures mental health, relationships and careers – and doctors who seem to have little idea what’s wrong with them.
Karen Ramage knew immediately after her endometrial ablation in 2021 that something wasn’t right.
The pain only got worse. The month prior, she had run 100 miles. By two weeks after the procedure, she couldn’t walk properly. She couldn’t drive, she couldn’t work, she could barely eat. And she couldn’t find a doctor who would agree the endometrial ablation might be to blame.
“My personal belief is that they just don’t expect anything to go wrong,” she told Sky News.
The discussion of risks beforehand was limited to being warned of adhesions between the womb and bladder or bowel, she says. She was told the worst outcome would be no improvement in her bleeding.
But constant pain set in down her right side, intensifying to “labour-like contraction pains” around the time of her period.
As months passed, she relied on daily doses of Tramadol. Talking to a counsellor, she tried to reckon with how she could live like this: “I felt that everything had been taken away from me.”
Karen Ramage had to pay for a hysterectomy privately after her ablation failed
It took going private for a doctor to tell her definitively her ablation had failed.
“I was probably more relieved that actually somebody would believe in me, because it was this whole thing that nobody would believe that this procedure had caused all of this.”
Facing up to a two-year wait on the NHS for a hysterectomy, she took out a loan to cover the £7,500 cost of having it privately. After months not working, it was a tough financial call – one that meant relying on food banks.
How ablations work – and fail
About one in four women suffer from heavy periods and more than 30,000 women in England had an endometrial ablation on the NHS between 2017 and 2022.
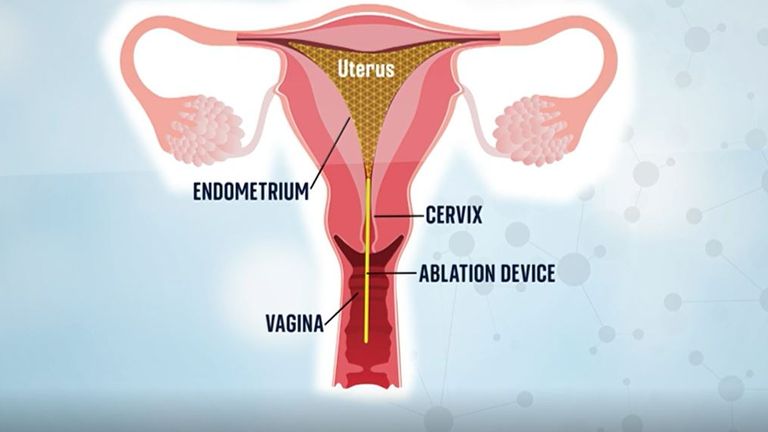
Most were radiofrequency ablations, where electromagnetic energy is used to burn away the lining of the womb.
The womb lining is what grows and sheds each month so the idea is that no lining means no – or lighter – periods.
But if not all the lining is destroyed, it still grows and sheds – but scar tissue can mean the blood gets trapped. It builds up in pockets behind the tissue, sometimes behind a scarred-shut cervix, causing intense pain until it disperses back into the body.
In women who have been sterilised the blood can back up into the fallopian tubes – this is known as PATSS (post-ablation tubal sterilisation syndrome).
In cases of late-onset failure, the lining regrows in the months and years after an ablation.
Some women experience pain cyclically each month, while for others post-ablation pain is constant or just during sex.
Women who spoke to Sky News describe agony worse than labour. One woman would put herself in the recovery position when the pain started because she knew she would blackout. Another came close to losing her job because she needed drugs so strong they made her a “zombie”.
‘Ablation ruined 10 years of my life’
Amanda Connor was told an ablation would “solve all my problems”, but three years later her womb had “completely grown back”. She decided to try the procedure a second time in 2010.
The pattern of monthly pain only intensified over time. It would start in her feet, a tingling fiery burn. By the time it reached her legs, she would be doubled over. Then it raged through her abdomen.
“I couldn’t stand up, I was on the floor writhing about and screaming for hours,” she told Sky News.
Her husband could only watch for so long before he would call an ambulance – just like he did the month prior, and the one before that.
At the hospital they would do the same checks for appendicitis, then pelvic inflammatory disease. But Amanda was sure they were looking for the wrong thing: “It’s not pelvic inflammatory disease, it’s happening every single month.”
Reports of not being believed or “gaslighting” were common among women who spoke to Sky News. One was told her pain must be a bladder infection. Two women were told it was IBS.
Nobody told Amanda it could be a failed ablation. She was the one who brought it up with her gynaecologist.
A scan revealed her womb was a “lump of scar tissue”. The only way to fix it was to remove her womb entirely.
She was shocked when her doctor told her: “Not only have I been totally misled about ablation and how amazing it is – I am now facing a major operation in order to fix it.
“If I could go back I would never have it done.
“Ablation ruined about 10 years of my life. The effect on my marriage, my work life and home life was huge.”
Taking legal action
Experiences like this are familiar to Dr Victoria Handley, a lawyer specialising in gynaecological medical negligence cases.
She estimates she’s handled about 1,000 cases relating to endometrial ablation since 2015. Every week she will hear from one or two women who have had complications from ablations.
They report adhesions of the uterus to the bladder or bowel, perforation of the uterus, infertility they weren’t warned about and ultimately needing further surgery.
Women are going to the doctor with heavy periods and ending up needing a hysterectomy, “the most radical thing you can have”, Dr Handley says. A hysterectomy carries risks including incontinence, sexual dysfunction, prolapse and early menopause.
“You’re swapping one problem for another without realising that the problem you’re swapping is actually worse than the problem you’ve got,” she told Sky News.

Dr Victoria Handley says she has handled about 1,000 cases
Exactly how many women suffer post-ablation complications is hard to pinpoint as research tends to only capture patients who have resorted to further surgery.
A study of more than 110,000 women in England who had an endometrial ablation between 2000 and 2011 found 16.7% had further surgery within five years. Other studies put the number at more than 20%.
Up to one in five ablation patients may have abnormal bleeding or period pain, or both, according to Professor Justin Clark, consultant gynaecologist and spokesperson for the Royal College of Obstetricians and Gynaecologists.
NICE guidelines set out treatment pathways for heavy bleeding. This includes taking a patient’s full history, investigating the cause of the bleeding and exploring conservative options like the coil and pill before an ablation.
A spokesperson for NHS England told Sky News staff should be following this guidance and “should make clear the benefits and potential risks of any recommended treatment so patients can make informed decisions”.
But Dr Handley says in her experience, “a lot of what’s in this guideline is ignored by the medical profession because they’ll go, ‘oh, I know what’s wrong with you’, and I’ll go straight to the surgery, and they don’t actually carry out the investigation and then send them down the correct route”.
Medical negligence cases need to establish a breach of duty; for endometrial ablation this is normally failure to warn of the risk of complications or failure to offer alternatives.
The claimant needs to prove they were injured, and the injury was caused by the breach. They also need to be able to show logically that had they been informed of the risks or alternatives, they would not have gone ahead with the ablation. If those four things don’t align, the case will fail, Dr Handley says.
The majority of cases are settled by NHS trusts out of court, she says, and women tend to receive upwards of £20,000, depending on the injury they have suffered.
Despite the number of cases she has dealt with, she says she has seen no attempt to solve the issue.
“The NHS response is woeful. There’s no joined up thinking at all. There’s no recognition that there’s an overarching problem, and there’s no desire to fix it.”
NHS England and NHS Scotland did not address questions from Sky News about how they are responding to this at an organisation-wide level.
‘It makes me sick to know my womb is burned’
Emma Burchell says she does not believe the risks were discussed in full when she had an ablation – which she calls “the worst decision I ever made”.
“You trust these doctors to do the right thing for you, and then you feel like they’ve not,” she says.
The months since the procedure in May 2022 have been “horrendous”. Constant sharp pain through her back, stomach and legs drove her to the doctor again and again, but she says she wasn’t given pain relief.
Instead she was offered antidepressants. She declined, worried she would be told the pain was “all in her head” if she accepted.
Now she’s considering a hysterectomy. “Do I need my womb?” she questions. “It makes me sick to know my womb is all burned, and it’s sat inside my stomach.”
But getting more surgery isn’t a quick fix. Gynaecological waiting lists in England have more than doubled since the start of the pandemic.
Emma has been put on injections to create a chemical menopause, a process which can help diagnose the cause of gynaecological symptoms, before doctors will consider a hysterectomy. In the meantime, each day is a “battle”.

Emma Burchell says getting an ablation was the ‘worst decision’ she’s ever made
Unsuitable candidates for ablation
A number of factors make an ablation more likely to fail: a younger age, fibroids, previous C-sections, polyps, a retroverted uterus (where the womb tips backwards) and adenomyosis (where the womb lining grows in the muscle of the womb).
According to Professor Clark, “endometrial ablation works best for women above 40 years old with relatively normal sized wombs without significant fibroids”.
Studies stress the importance of making sure women are good candidates for the procedure. A medical device alert from the UK’s Medicines and Healthcare products Regulatory Agency said the same.
Still, Sky News spoke to women who between them had all the contraindications above and had been given an ablation.
Karen Ramage found out after her ablation that she had a retroverted uterus – increasing the chance of ablation failure sixfold – as well as fibroids.
Ablations can be done where women have small fibroids, but she was told in her case it was like trying to “wallpaper over air bubbles and lumps, so it doesn’t cover the whole surface”.
When ablations work
Endometrial ablation support groups have sprung up on Facebook; the largest has more than 14,000 members, mostly in the US.
Women share stories of nerve damage, sepsis, infections, bloating, continued heavy bleeding. It’s nerve wracking reading for people considering the procedure – or who had it done before finding the group.
Samantha Williams hovers in the group, popping up in the comments to share her experience and reassure people. She had an ablation after 18 months of non-stop bleeding and it made a “massive difference” to her quality of life. It stopped the bleeding and hasn’t caused pain.
Read more on Sky News:
New workplace standards for menopause and menstruation support
Women more likely to suffer migraines during menstrual cycle
If you think of treatments for heavy bleeding as the alphabet, she says, a hysterectomy is Z. With her NHS gynaecologist they worked through until they got to Y, an ablation.
The risks were explained, the patient information leaflet was detailed and she was confident it was right for her.
Still, her advice is the same as women who had bad experiences: “Do your homework. But also try everything else first. It shouldn’t ever be the first thing that you do. There’s lots of other options.”
What the NHS says
Sky News contacted NHS England and Scotland, as well as the NHS trusts that treated Karen, Amanda and Emma.
NHS England said endometrial ablation is “one of a number of treatments” for heavy bleeding that is given “when clinically appropriate”.
“While most women do not experience significant pain after this procedure, we strongly encourage any woman with concerns to speak to their clinician or GP,” it said.
A Scottish government spokesperson said “person-centred care” was a priority and involved working in partnership with patients to understand what they need, and how their desired outcomes can be achieved.
“An essential component of this approach involves providing tailored, understandable information so that people are fully informed and involved in decision-making about their care as much as they choose.”
A spokesperson for Bolton NHS Foundation Trust said: “We welcome the opportunity to speak with any patient directly if they had concerns about their care or treatment, so we can fully understand their experience and make improvements where possible.”
NHS Forth Valley again said it followed guidelines and best practice, adding that treatment options may be discussed at multidisciplinary team meetings to identify the most suitable options.
Follow up investigations would be carried out where there is ongoing pain or other symptoms, which could identify unrelated medical conditions as the source of pain, the spokesperson said.


The ringleader of a Romanian grooming gang was offered £1,500 by the Home Office to be deported while he was in prison awaiting trial for 10 rapes, a Sky News investigation has found.
Mircea Marian Cumpanasoiu, 38, led a network which raped, drugged and exploited vulnerable local women in Dundee.
But Sky News can exclusively reveal that in summer 2024, while in custody at HMP Perth awaiting trial for serial sex offences, officials handed him a “voluntary return” form under a government scheme paying foreign nationals to leave Britain.
The department later decided not to remove him because of the upcoming court proceedings.
Immigration status renewed during trial
In another twist, just months later – as he stood in a High Court dock facing 10 rape charges – Sky News has discovered Cumpanasoiu’s immigration status, which was due to expire, was automatically renewed under the EU settlement scheme.
Cumpanasoiu was later handed a 24-year extended sentence, with 20 years in jail and four on licence, for sexual and trafficking offences.
Cumpanasoiu winking to the camera during a video filmed near a brothel in Dundee. Pic: Crown Office
Prosecutors described him as a “winking, smirking pimp” who once filmed a victim climbing a tree to escape his anger when she “failed” to make enough money in Dundee brothels.
Following days of questions from Sky News, officials have confirmed his settled status has now been revoked.
The inside story
Sky sources say Home Office workers personally met Cumpanasoiu at Perth prison while he was on remand in August 2024.
Sources say he “expressed a desire to return home” and was handed documents to sign agreeing to a cash-assisted return, but the plan was later blocked.
But in another twist, on 2 December 2024, halfway through the grooming gang trial, his EU settled status was renewed.
A source close to proceedings told Sky News the revelations “smack of incompetence”.
The Home Office does not dispute this version of events.

Romanian grooming gang clockwise from top left: Remus Stan, Alexandra Bugonea, Mircea Marian Cumpanasoiu, Cristian Urlateanu and Catalin Dobre. Pics: Police Scotland
Rape Crisis Scotland said the case raises concerns.
A spokesperson for the charity said: “This was a horrific case, which involved numerous vulnerable survivors who showed tremendous strength and courage by coming forward to seek justice for what had happened to them.
“The severity of this case has, quite rightly, resulted in significant prison sentences for the perpetrators. However, it is not clear why the Home Office tried to intervene before a trial had begun, and any verdict had been reached.
“Survivors must have faith in the criminal justice process and its ability to hold perpetrators accountable for their crimes.
“This incident raises questions about what the Home Office’s intentions were, and why it was able to insert itself into active criminal proceedings in the first place.”
Read more from Sky News:
Swinney ‘open’ to national inquiry into grooming gangs
Why are abuse survivors losing faith in grooming gang inquiry?
What is the EU Settlement Scheme?
The EU Settlement Scheme was set up after Brexit to allow citizens from the EU, and their family members, to continue living and working in the UK.
People with “settled status” can stay in the UK indefinitely.
Those with “pre-settled status”, such as Cumpanasoiu, must reapply after five years.
Since September 2023, the Home Office has introduced automatic extensions of pre-settled status which means renewals happen electronically unless officials intervene.
There are questions now about whether this automation can lead to offenders such as Cumpanasoiu being overlooked.
Home Office ‘had power to intervene’
Jen Ang, a human rights lawyer and leading expert on migrants’ rights, told Sky News the vast majority of those processed under the EU system are law-abiding citizens.
But Ms Ang, a professor at the University of Glasgow, reveals authorities did have the power to intervene in this case.

Professor Jen Ang
She said: “In this case the Home Office did have the power and the right to stop the automatic renewal. At any point where it is possible that someone is about to become unsuitable for settled status, the Home Office could have intervened.
“The optics of this in the context of such a high-profile and horrific crime are not great.”
‘The public are entitled to be concerned’
Thomas Leonard Ross KC, a leading Scottish defence lawyer, described the decision-making as “flawed”.
He said: “I mean automatically renewing pre-settled status in 99.9% of occasions can be done without any risk to the public. But clearly this particular individual has been assessed to be an extremely dangerous person.
“The public are perfectly entitled to be concerned. A decision of this type made automatically without any assessment as to the risk that he might pose is clearly a flawed decision.”
A Home Office spokesman said: “This man will serve his sentence for the abhorrent crimes he committed and will be considered for deportation at the earliest opportunity.
“A deportation order will automatically trigger the revocation of an individual’s right to be in the UK, including pre-settled status.”


The novel has survived the industrial revolution, radio, television, and the internet. Now it’s facing artificial intelligence – and novelists are worried.
Half (51%) fear that they will be replaced by AI entirely, according to a new survey, even though for the most part they don’t use the technology themselves.
More immediately, 85% say they think their future income will be negatively impacted by AI, and 39% claim their finances have already taken a hit.
Tracy Chevalier, the bestselling author of Girl With A Pearl Earring and The Glassmaker, shares that concern.
“I worry that a book industry driven mainly by profit will be tempted to use AI more and more to generate books,” she said in response to the survey.
“If it is cheaper to produce novels using AI (no advance or royalties to pay to authors, quicker production, retainment of copyright), publishers will almost inevitably choose to publish them.
“And if they are priced cheaper than ‘human made’ books, readers are likely to buy them, the way we buy machine-made jumpers rather than the more expensive hand-knitted ones.”
Chevalier, author of the book Girl With A Pearl Earring, with the painting of the same name. Pic: AP
Why authors are so worried
The University of Cambridge’s Minderoo Centre for Technology and Democracy asked 258 published novelists and 74 industry insiders how AI is viewed and used in the world of British fiction.
Alongside existential fears about the wholesale replacement of the novel, many authors reported a loss of income from AI, which they attributed to “competition from AI-generated books and the loss of jobs which provide supplementary streams of income, such as copywriting”.
Some respondents reported finding “rip-off AI-generated imitations” of their own books, as well books “written under their name which they haven’t produced”.
Last year, the Authors Guild warned that “the growing access to AI is driving a new surge of low-quality sham ‘books’ on Amazon”, which has limited the number of publications per day on its Kindle self-publishing platform to combat the influx of AI-generated books.
The median income for a novelist is currently £7,000 and many make ends meet by doing related work, such as audiobook narration, copywriting or ghost-writing.
Read more: The author embracing AI to help write novels

Could the AI bubble burst?
These tasks, authors feared, were already being supplanted by AI, although little evidence was provided for this claim, which was not possible to verify independently.
Copyright was also a big concern, with 59% of novelists reporting that they knew their work had been used to train AI models.
Of these, 99% said they did not give permission and 100% said they were not remunerated for this use.
Earlier this year, AI firm Anthropic agreed to pay authors $1.5bn (£1.2bn) to settle a lawsuit which claimed the company stole their work.
The judge in the US court case ruled that Anthropic had downloaded more than seven million digital copies of books it “knew had been pirated” and ordered the firm to pay authors compensation.
However, the judge sided with Anthropic over the question of copyright, saying that the AI model was doing something akin to when a human reads a book to inspire new work, rather than simply copying.
Read more from Sky News:
Scientists sound alarm over ultra-processed foods
‘What is it really like being a British journalist in Moscow?’
Most novelists – 67% – never used it for creative work, although a few said they found it very useful for speeding up drafting or editing.
One case study featured in the report is Lizbeth Crawford, a novelist in multiple genres, including fantasy and romance. She describes working with AI as a writing partner, using it to spot plot holes and trim adjectives.
“Lizbeth used to write about one novel per year, but now she can do three per year, and her target is five,” notes the author of the report, Dr Clementine Collett.
Is there a role for government?
Despite this, the report’s foreword urges the government to slow down the spread of AI by strengthening copyright law to protect authors and other creatives.
The government has proposed making an exception to UK copyright law for “text and data mining”, which might make authors and other copyright holders opt out to stop their work being used to train AI models.
“That approach prioritises access to data for the world’s technology companies at the cost to the UK’s own creative industries,” writes Professor Gina Neff, executive director of the Minderoo Centre for Technology and Democracy.
“It is both bad economics and a betrayal of the very cultural assets of British soft power.”
A government spokesperson said: “Throughout this process we have, and always will, put the interests of the UK’s citizens and businesses first.
“We’ve always been clear on the need to work with both the creative industries and AI sector to drive AI innovation and ensure robust protections for creators.
“We are bringing together both British and global companies, alongside voices beyond the AI and creative sectors, to ensure we can capture the broadest possible range of expert views as we consider next steps.”


They’ve said they are offering him an opportunity to tell them everything, once and for all.
But as we hit the two-week deadline set by the US Congress committee investigating Jeffrey Epstein for a reply from Andrew Mountbatten-Windsor, will he agree to their request to open up about the paedophile financier?
The letter sent by the House Committee on Oversight and Government Reform said members wanted to talk to him because of the widely reported allegations that have been made against him, which he denies, and because of his relationship with Epstein and what he may have seen.
The committee is looking into Epstein’s crimes and his wider sex trafficking network. Andrew was given until today, 20 November, to respond.
Legally he isn’t obliged to talk to them, and to be honest it’s hard to imagine why he would.
The only time he has spoken at length about the allegations against him and his relationship with Epstein was that Newsnight interview in 2019, and we all know how much of a disaster that was.
Releasing the Epstein files: How we got here
Yes, this could be an opportunity for him to publicly apologise for keeping up his links with Epstein, which he has never done before, or show some sympathy towards Epstein’s victims, even as he vehemently denies the allegations against him.
But while there is the moral argument that he should tell the committee everything he knows, it could also raise more uncomfortable questions for him, and that could feel like too much of a risk for Andrew and the wider Royal Family.
However, even saying no won’t draw all this to a close. There are other outstanding loose ends.
The Metropolitan Police still have to tell us if they intend to take any further action after they said they were looking into claims Andrew had asked one of his officers to dig up dirt on his accuser, Virginia Giuffre.
Read more:
King formally strips Andrew of prince title
Bill to release Epstein files gets all-clear from Congress

The new Epstein files: The key takeaways
There could also still be a debate in parliament about the Andrew problem.
The Liberal Democrats have said they want to use their opposition debating time to bring the issue to the floor of the House of Commons, while other MPs on the Public Accounts Committee have signalled their intention to look into Andrew’s finances and housing arrangements.
And then there are the wider Epstein files over in America, and what information they may hold.
From developments this week, it seems we are edging ever closer to seeing those released.
All of this may mean Andrew in other ways is forced to say more than he wants to, even without opening up to the Congress committee.
-
 Sports2 years ago
Sports2 years agoStory injured on diving stop, exits Red Sox game
-
 Sports3 years ago
Sports3 years ago‘Storybook stuff’: Inside the night Bryce Harper sent the Phillies to the World Series
-
 Sports2 years ago
Sports2 years agoGame 1 of WS least-watched in recorded history
-
 Sports3 years ago
Sports3 years agoButton battles heat exhaustion in NASCAR debut
-
 Sports3 years ago
Sports3 years agoMLB Rank 2023: Ranking baseball’s top 100 players
-
Sports4 years ago
Team Europe easily wins 4th straight Laver Cup
-
 Environment2 years ago
Environment2 years agoJapan and South Korea have a lot at stake in a free and open South China Sea
-
 Environment1 year ago
Environment1 year agoHere are the best electric bikes you can buy at every price level in October 2024